What we do as a Network
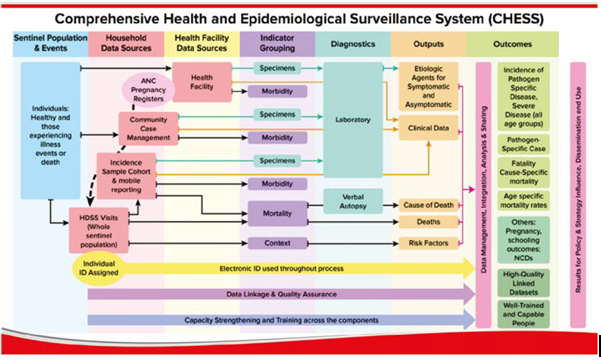
Above chart shows INDEPTH in the near future - implementing CHESS, Lancet Global Health 2015
We conduct longitudinal research based on Health and Demographic Surveillance System (HDSS) field sites in low- and middle-income countries (LMICs) to improve the lives of people in these countries by informing and influencing policy.
We provide robust answers to some of the most important questions in development.
Through our global network of HDSS field sites in Africa, Asia and Oceania, we are capable of producing reliable longitudinal data not only about the lives of people in LMICs, but about the impact on those lives of development policies and programmes.
We are now implementing a new generation of population surveillance operations—the Comprehensive Health and Epidemiological Surveillance System (CHESS)—capable of timely delivery of high-quality data for disease-specific and pathogen-specific morbidity, together with data for overall and cause-specific mortality.
In addition to disease causes and morbidities, CHESS includes full risk factor surveillance and address the full range of the rapidly transitioning burden of disease, including non-communicable diseases and external causes and their associated morbidities. Importantly, CHESS includes monitoring health systems and policy initiatives because they affect communities and households.
In implementing CHESS, we do not underplay the importance of documentation, study, and implementation of intervention studies related to inequalities in health, health-care access and use, and intervention coverage. CHESS will be founded on established dynamic cohort surveillance approaches, by building on existing methods used in health and demographic surveillance systems (HDSSs).
The main CHESS innovation is integration across population and health facility data systems, linking demographic, epidemiological, mortality, morbidity, clinical, laboratory, household, environmental, health systems, and other contextual data, with a unique electronic individual identification system throughout. This integration generates empirical unbiased data essential for development and assessment of interventions at the subnational level. Data from health facilities are linked to community-level information. For example, mortality data are collected both from health facilities (with medical certificates of cause of death) and from the community, through verbal autopsy.
Subcohorts within CHESS populations are followed up to monitor morbidity incidence and collect clinical data and laboratory specimens, through frequent scheduled household visits (active surveillance) and unscheduled visits triggered by mobile phone contacts from households. Additionally, sentinel health facility data provide information about severe diseases and their causes, with outcomes traced back to household levels on a timely basis. CHESS provides numerators and denominators for population-based diseases with causes and mortality disaggregated by finely specified age groups (including neonates).
The HDSS foundation for CHESS is enhanced by crucial innovations needed for the morbidity and aetiological surveillance components, at both household and health facility levels. Household-based cohort studies with an electronic illness notification system, in addition to operational and data linkages with health facilities, are complemented by advanced quality-assured clinical and laboratory investigations and expertise.
Data collection for CHESS builds on existing HDSS platforms, thereby making unique identifiers (either electronic or biometric) available for every individual. These identifiers also have the potential to be linked to national identification systems, which is necessary for integration of datasets from households, health facilities, and laboratories. CHESS uses technological solutions to establish an integrated electronic surveillance system combining all relevant data sources and allowing for appropriate response. CHESS provides complementary data to national health management and information systems and link to local civil registration systems, enabling access to birth and death registration and certification for the population, and thus providing individuals and families with direct benefits.
We are aware that the above enhancements need substantial developments in resources, expertise, and capacity, and will have substantial opportunity costs. Robust ethical safeguards also have to be considered. However, now is the moment to firmly state that the world cannot continue to work without essential and large-scale population health information.
HOW WE WORK AS A NETWORK THROUGH THE INDEPTH RESOURCE & TRAINING CENTRE
- We support the INDEPTH Working Groups to realise their ambitious plans for expanding the boundaries of scientific knowledge based on HDSS research.
- We strengthen the capacities of HDSS members and train their staff to conduct high quality health and demographic research.
- We enhance members’ scientific productivity and improve on the quality of data collection, analysis and management.
- We focus on building a pool of highly trained and efficient young researchers/scientists to conduct world-class research and ensure sustainable leaders for the respective HDSSs.
- In partnership with our collaborators, we energetically strive to translate the successful research into improved global policies. To this end, we synthesise the knowledge generated by INDEPTH into comprehensive policy documents to influence policy-making and ensuring an on-going dialogue among policy makers, practitioners and scientists.
- We always seek and use every opportunity to work closely with the Board of Trustees who in turn demonstrates its leadership role.
- We utilise the Scientific Advisory Committee to steer the Network’s scientific agenda into promising directions.